
Previous post



Rationed by race. That is how far too many hospitals and states are rationing treatment of those ill with Covid. In other words, the criteria for care now has race at the forefront.
In New York, racial minorities are automatically eligible for scarce COVID-19 therapeutics, regardless of age or underlying conditions. In Utah, “Latinx ethnicity” counts for more points than “congestive heart failure” in a patient’s “COVID-19 risk score”—the state’s framework for allocating monoclonal antibodies. And in Minnesota, health officials have devised their own “ethical framework” that prioritizes black 18-year-olds over white 64-year-olds—even though the latter are at much higher risk of severe disease.
These schemes have sparked widespread condemnation of the state governments implementing them. But the idea to use race to determine drug eligibility wasn’t hatched in local health departments; it came directly from the federal Food and Drug Administration.
Think about that. Instead of hospitals running actual triage based upon what the patient’s medical situation is, they will be running triage based upon race.
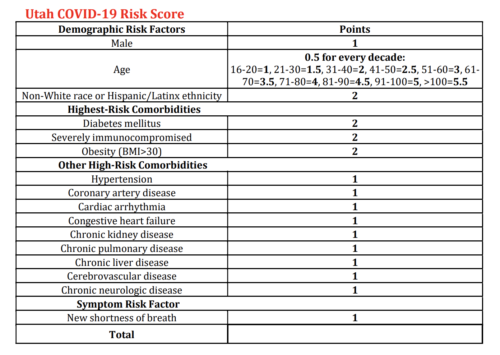
Photo credit: Graph via Washington Free Beacon
In a normal world, this would be called discrimination. In a normal world, people would be spitting fire that medical care can only be received if one checks the appropriate race boxes. Instead, as we’ve seen for the last two years, the normal RATIONAL world has been upended.
We are now supposed to offer medical care that is ‘equitable,’ ‘fair’ and checks all the social justice boxes.
In New York, medical practitioners are supposed to consider race and ethnicity when determining who is eligible to receive life-saving therapeutics and/or monoclonal antibodies. They bluntly state that Covid treatment preference MUST be given to those who are Native American, Black, or people of color. Only one big problem with that.
Far and away the most significant factor associated with severe COVID-19 disease and death is age. Taking the 18-39 age group as a reference (Risk Ratio of 1), the risk of death doubles for the 40-49 age group (RR=2.2), doubles again in the 50-64 group (RR=4.3), and reaches an RR of 6.7 for those 65-74. The RR tops out for those 85 and older at 10.6.
What’s even worse is that New York and other states are now prioritizing distribution of Covid treatments by ZIP CODE.
As the nation prepared to roll out vaccines in fall 2020, the Centers for Disease Control and Prevention called on states to submit their distribution plans. That September, the agency urged them to prioritize disadvantaged populations, including “people from racial and ethnic minority groups,” for vaccine supplies and appointments, instead of spreading the resources equally. Thirty-four states complied.
~Snip
It’s one thing to wait for a vaccine or a test kit; it’s another to go to the back of the line for an ICU bed or ventilator. In April 2020, in response to the pandemic, the University of Pittsburgh Department of Critical Care Medicine adopted a plan for triaging critically ill patients when beds and ventilators run low.
Patients get a score based on their likelihood of survival, considering their organ function and other illnesses. But instead of allocating critical care based only on this, Pitt now adds a “correction factor,” dependent on the patient’s ZIP code. Patients from the most disadvantaged neighborhoods will get their scores increased, leapfrogging ahead of others with the same medical conditions.
This as the Biden Administration has continued to fail at their roll out of vaccines, has ensured that there is now a shortage of test kits, and hospitals such as the Mayo Clinic are shortchanging healthcare by firing anyone who isn’t fully (4 or is it 9 jabs) vaccinated. States such as Florida have quit relying on the federal government to get tests and treatments into the states. Instead, they’ve been going directly to the manufacturers and distributors.
If this guidance had been implemented during the Trump Presidency, what do you think the reaction would be? Epically nuclear would be my guess. The shrill screams of discrimination combined with the stern opining from the pundits would be going on for MONTHS. And that doesn’t take into consideration the plethora of lawsuits that would’ve been filed at all levels.
Instead, because it is the Biden Administration, the mainstream media is saying nothing. The politicians are silent, and all the pundits have zipped their lips.

Discrimination is AWESOME when the Biden Administration is in town.
NY State Department of Health warns they don't have enough Paxlovid or Monoclonal Antibody Treatment and white people need not apply. https://t.co/shbMWDomLJ pic.twitter.com/MwBtjv2pDx
— Karol Markowicz (@karol) December 31, 2021
And, if that means that discrimination ends up with a white person dying while that person of color got treatment? So be it.
The American government is now denying medial treatment to individuals based on race. That's what happens when critical race theory becomes public policy.
— Christopher F. Rufo ⚔️ (@realchrisrufo) January 7, 2022
For this type of discrimination to be welcomed into our healthcare system is hideously wrong and medically dangerous to our public health.
Feature Photo Credit: Doctor, surgery photo via Pixabay, cropped and modified


[…] post Covid Treatments Rationed By Race appeared first on Victory Girls […]
Hmmm….Government agencies practicing racism; who woulda thunk?
Odd that such things seem much more prevalent when democrats are running things…
It’s almost as if they’re the virulent racists that they accuse conservatives of being…
I saw it when I was trying to set up an appointment for my shots.
“Race?”
“Human.”
“That’s not on here. Ethnicity?”
“American.”
Sounds of exasperation. “Are you a white non-Hispanic?”
“Is that *really* going to determine whether or not I get an appointment?”
Thankfully, the little drone didn’t push the issue.







{kind=link}
4 Comments